

Relief for Dallas Health & Human Services Dept.
Overview
I conducted seven research protocols for Dallas County Health and Human Services (HHS)
I researched, collaborated, and presented patient experiences from the Refugee Health Services Clinic to Dallas County team for an optimized patient workflow.
My Roles
UX Researcher/Designer and Project Manager
Partners
Dallas County - Refugee Health Services, International Rescue Committee
Topics
Healthcare, Service Design, Social Work and Customer Experience
The Challenge
2 of the top 10
largest refugee clinics nationwide are located in Texas.
Dallas County Health and Human Services Records, 2024
~9,600 patients
are seen yearly at the Refugee Health Services clinic in Dallas County
Dallas County, 2024 estimate
Refugees arrive into a dense, fragmented network of clinics, caseworkers, and localized community organizations. The gap isn't effort — it’s coordination.
I needed to gauge the existing services provided by HHS and external partners in the process of resettling families
The Process
-
Background Research
Research on public health and current resources offered to partners and more
-
Surveys & Interviews
Research guides for the partners to engage and serve patients
-
Workshop & Market Research
I engaged stakeholders in research to gauge pain-points and gaps in services
-
Prototype & Next Steps
I developed a set of recommendations for the county and how to scale the product
Background Research
I empathized with patients to understand their needs in the medical resettlement process
To provide a specific boundary of focus, I used three of the seven components of whole health for refugees and their resettlement needs in DFW to best frame my scope/impact
My initial research of mapping the support network(s) came from the following two focus areas
Lived Experiences of Health Experts
I interviewed the following medical staff in Dallas County Refugee Health Services Clinic:
2 Clinic Managers
4 Registered Nurses
1 Reception Staff
1 Community Health Assistant
Local Patient Needs
Structured evaluation of patient needs was reviewed by an observation of:
Health Systems in DFW
Resettlement Services
Issues With Medical Visits.

Family Onboarding Process - A supportive perspective
Providing care to a newly arrived family is a legal and medical process, the screening, arrival and resettlement are all a part of showing attention, respect, and care for refugees traveling from home to home
Surveys and Interviews
I coached 3 HHS medical staff on design research, data collection methods, and reporting for an ideal outcome.
Via observation of current appointment scheduling, patient use of transit systems, medical resettlement services, and observing health visits by refugees I understood the scale of issues and what limitations each internal team.
The two research protocols shared by myself and the HHS team resulted in the following three insights
-
I sought to test out the following topics via this experiment
Patient Communication Gauge
Modality and Messaging
-
This interview sought out to explain the following:
Patient Appt. Scheduling Process
Scheduling Modality and Effectiveness
Appointment Preference
Patients preferred full family-oriented medical services over multiple individual visits
Insight derived from +3 hours of interviews with clinic managers
System-wide Care
Refugees felt like some programs were rushed or impersonal outside of the HHS services
Insight derived from four patient interviews at the HHS clinic
Accessibility of Services
Refugees had inconsistent awareness of services provided inside and outside of HHS
Insight derived from +6 HHS staff and patient interviews
Working with case managers, other clinics, and support staff showed me that the underlying issues were due to triage and alignment of services between organizations.
Initial Insights:
After +18 hours of interviewing caseworkers, clinic managers, and +45 new/current patients I found the need to host a workshop.
Workshop and Market Research
I helped non-profits, clinics, school districts and other community members align services
Learning about federal and state updates during the Quarterly Refugee resource planning meeting I was able to further understand the strategic priorities of non-profits, clinics, school districts and other community members
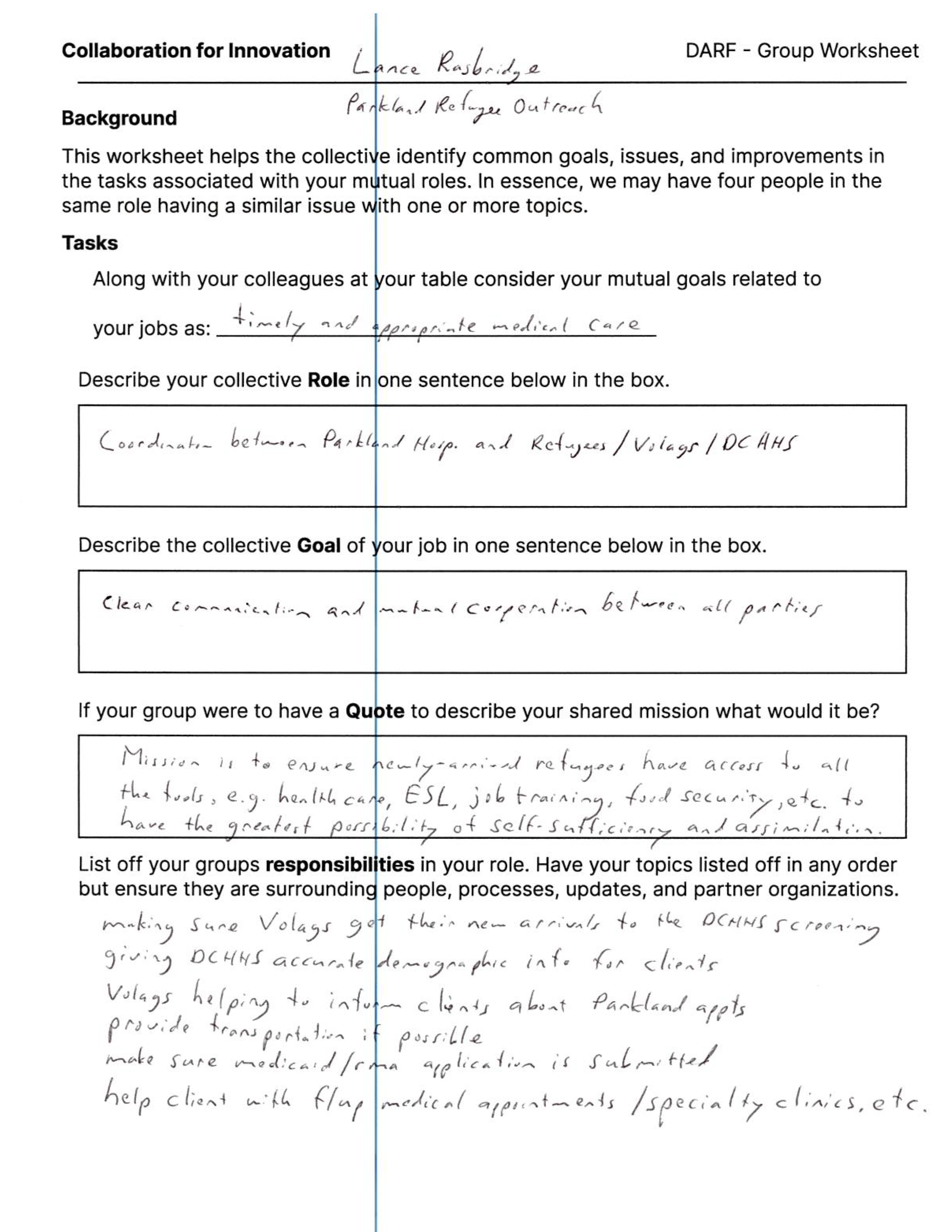
What would bring shared value to the individual orgs and project?
Unified Vision - Align perspectives of resettlement agencies, non-profits, and medical orgs
Collective Mission - Re-define and reinforce common goals in the resettlement process
Community Organization - Map roles in establishing new arrivals into the DFW community
I had three overall goals for the workshop which would group together members from each organization and optimize collaboration
Workshop Goals:
Health Network Insights
Community Resources
Supporting clients, care networks, and caseworkers in the DFW area with a single platform
Resource Portal — unified resources, providers, and more
Communication — Simple and consistent area of information
Health Network Insights
Workshop Documentation - Sample
Partners in Progress


Caseworkers were the most critical to providing quality social, medical, and career engagement for refugees and families.
I felt the need to come up with a blue sky idea that would serve both resettled clients and the caseworkers in the resettlement process.
Resettlement Process
Caseworker/patient tasks and procedures were expanded to include additional teams
Medical Needs — appointments, records, and follow-ups
Educational Steps — speaking to the impact of each process

Focus on Caseworkers
The caseworkers were established as critical people to providing quality medical services and engagement
Caretaking — serves others via community, housing, and more
Wayfinding — helping in the navigation of unfamiliar systems

Mariana — Resettled Client
Newly arrived, navigating unfamiliar systems
Medical needs — appointments, records, follow-ups across providers
Social needs — community, family security, language access, and emotional support
Relocation needs — housing, transportation, orientation in her new city
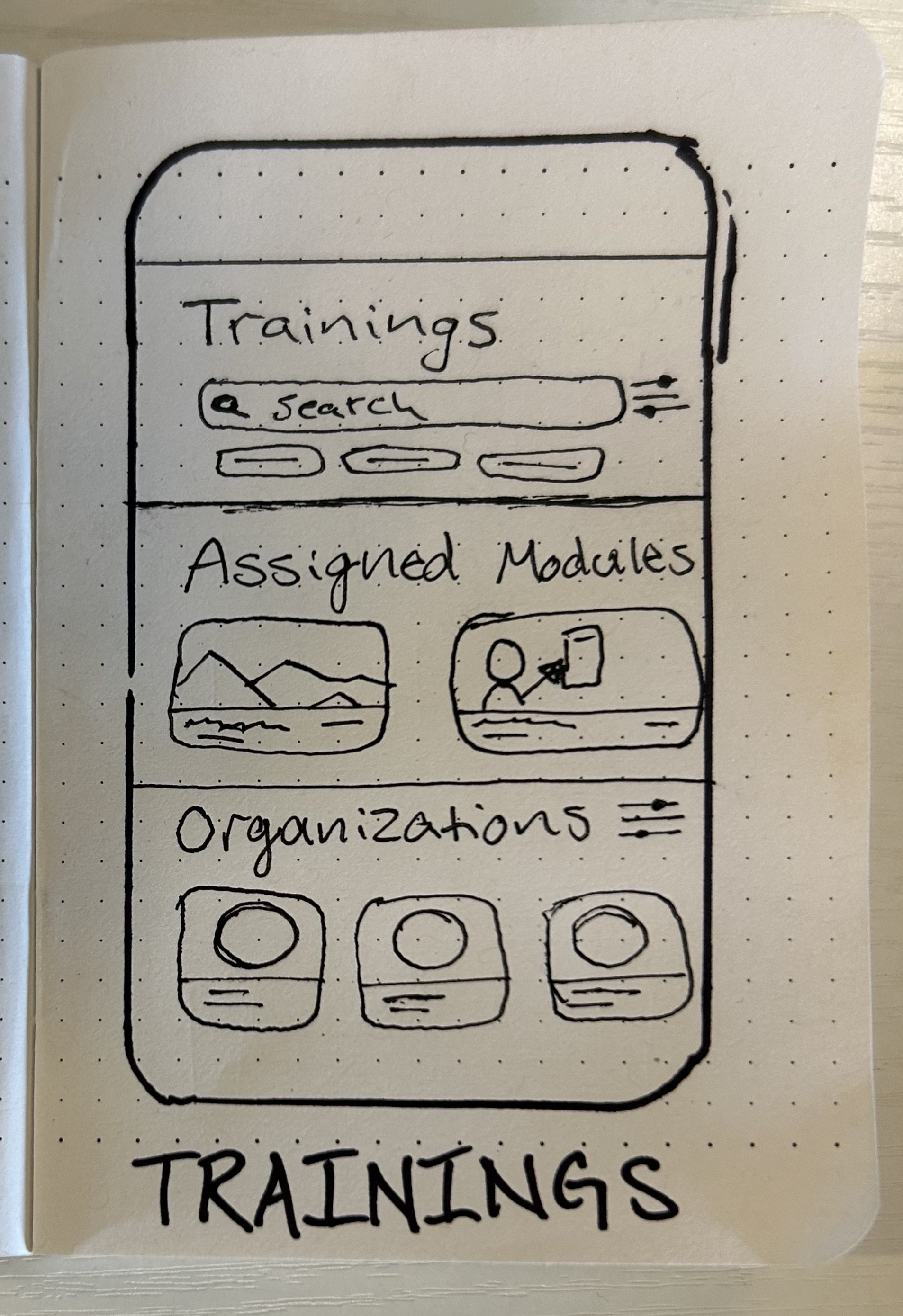
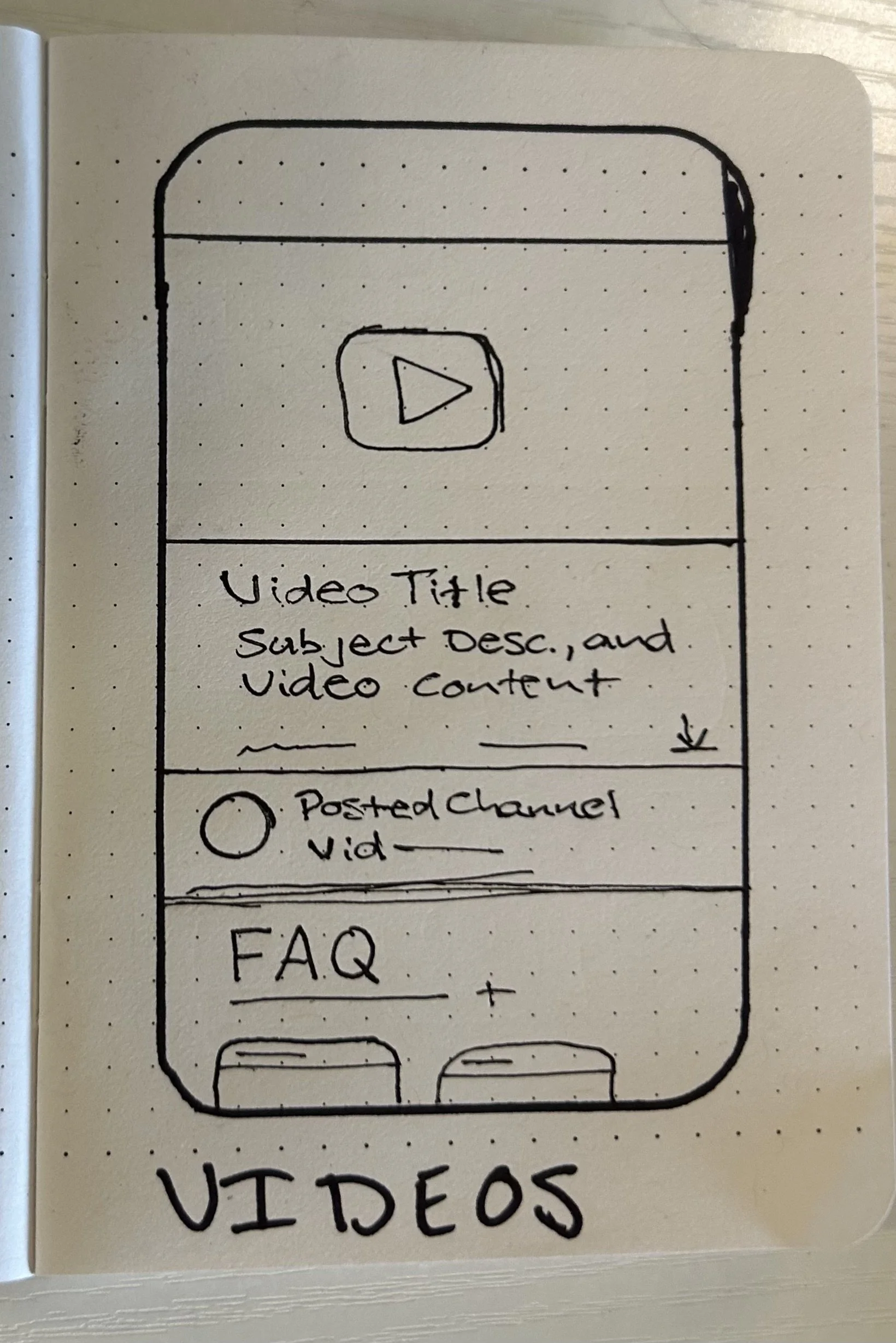
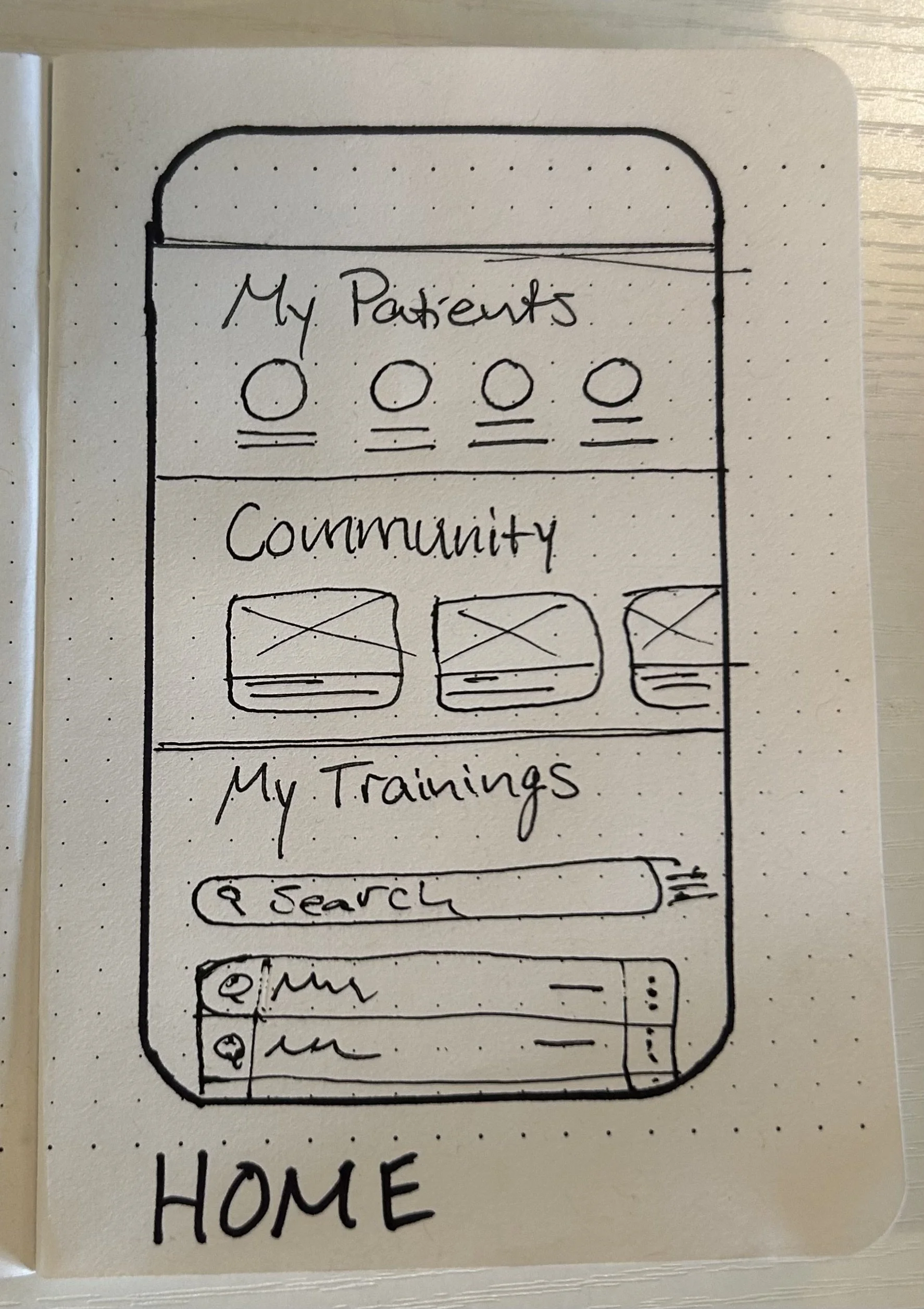
Wireframes for caseworker mobile Relief training module
Ariel — Resettlement Caseworker
Managing a high-volume caseload across multiple agencies
Internal Documentation — intake, updates, and managing secure records
External organizations — coordinating across clinics, NGOs, and county services
Mass monthly caseload — staying on top of dozens of active client needs at once
Workshop Output - Refugee EMR Platform
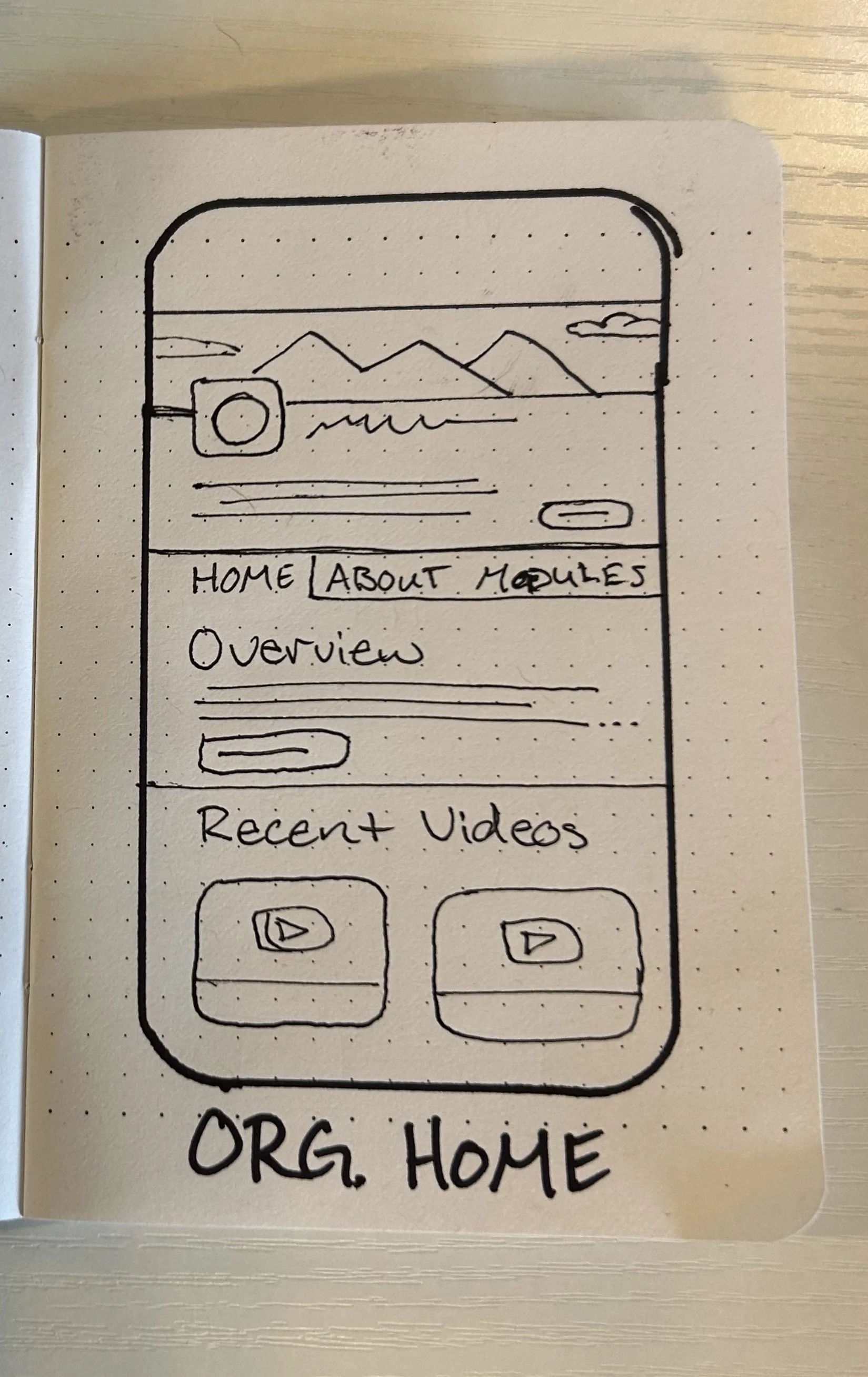
Wireframe for refugee home page and NGO public profile

Developing a multi-sided (provider, caseworker, and patient) platform would be ideal for an optimized hand off of services, information, documentation, and identifiable gaps in services between NGOs and health systems in the resettlement process
A unified platform that manages medical records, trainings, and community resources can alleviate the load for medical providers, caseworkers and new arrivals to DFW .
Prototype and Next Steps
A go to market strategy was made for the Relief app using research insights to improve the resettlement experience
Go To Market Strategy - Relief
What industries would be interested in resettlement management?
Education - Testing benchmarks and school year attendance records/requirements of new students
Hospital Networks - Appointment scheduling and timely arrivals of patients and new/previous medical records
Non-Profits - Ease of management, retention, and success of caseworkers/respective caseload
$1.78M available
with ¾ of the workshop participants
Use Case Validation
100% positive reviews were given during the walkthrough with 2 caseworkers and a medical provider in the HHS team.

Re-establishing caseworker training into a centralized platform gives organizations increased engagement and visibility with each respective team mate in the process
-
Care Network Engagement
Client, Provider, and Caseworker Portals
Medical and Support Onboarding for refugees/resettled populations
Using available data, established product features in market, resettlement KPIs, and feedback from the workshop, the GTM included three currently interested markets for a five year implementation of a customized EMR services implementation
Relief as a concept would have been unrealistic at the time, DHHS staff were instructed to take the research outcomes and develop video training modules on for their partners using existing tools
What I learned
-
Building a vision of research and collective mission is immeasurable in invaluable for teams that are new to design strategy
Leadership and Support
-
Group research should prioritize consistency, team feedback, and the ability to iterate on relevant data gathering tools/structure
Data Capture Tools
-
Brining together external partners always requires extra time, planning, and a shared value proposition to ensure participation
Partner Engagement
Other Projects


Living and Driving Safety for Elders
